How many healthy years can you actually buy?
You're 51. You run a company, or you sold one. You exercise four times a week, sleep well most nights, and eat reasonably. By any standard measure, you're in good health. But last year a friend your age was diagnosed with pancreatic cancer - stage three, caught late. And now there's a question you can't shake: what could I actually be doing to catch something like that early?
You look into it. A full-body MRI, advanced bloodwork, a cardiac CT scan - just to know. You're not anxious, you're being rational. And you're perfectly willing to pay. But in the Netherlands, willingness isn't enough. Your GP sees no indication, the specialist won't see you without a referral, and the scan you want isn't covered. Getting it privately feels like navigating a system that would rather you didn't. Not because anyone disagrees with what you're trying to do, but because the system simply wasn't built for it.
From purchasing power to healthy years
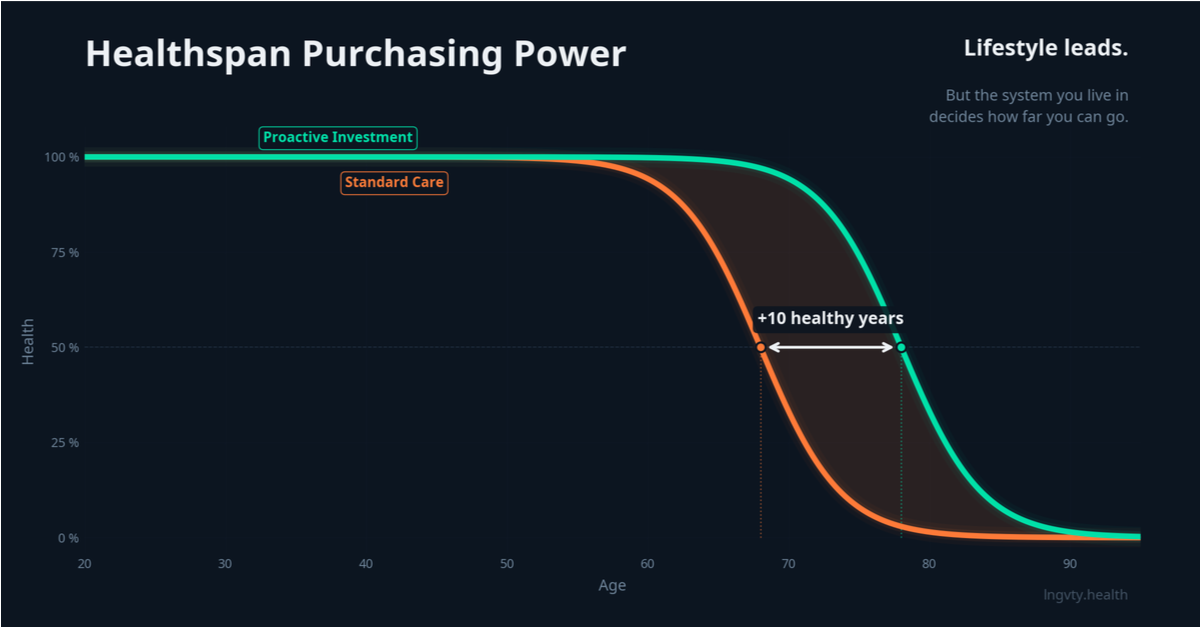
Every year in the Netherlands, we debate purchasing power. Will households have more or less to spend next year? It dominates political conversation. But purchasing power tells you nothing about what that money can actually do for your health. Which raises a different, increasingly relevant question: how many healthy life years can you actually buy with your disposable income?
This is what we call Healthspan Purchasing Power — the degree to which you can convert income into longer, healthier living, given the pricing, regulation, and access available to you. It's not about how much care exists in a country. It's about what you, as an individual, can meaningfully act on.
What this looks like in practice
Consider three people with similar incomes and similar intentions - one in the Netherlands, one in the United States, one in Singapore. In the Netherlands, someone concerned about cardiovascular risk faces a months-long path: a GP conversation, possibly a referral, then a wait. A coronary calcium score - ten-minute CT-scan - isn't part of standard screening, and getting one privately is possible but opaque. In the United States, that same person can walk into a preventive health clinic next Tuesday, pay out of pocket, and have results by Thursday. Physicians have more latitude to order diagnostics and act on early signals. The access is real, but so is the inequality. In Singapore, preventive screening is culturally normal. A full executive health panel including advanced imaging and biomarkers is routine, affordable, and socially unremarkable. Individual choice fits naturally within the system rather than pushing against it. The medical knowledge across all three countries is roughly the same. The difference is in what you're allowed and able to do with it.
A distinctly Dutch opportunity
The Netherlands doesn't need to become a country where only the wealthy can age well. But nor does it need to remain a system where everyone follows exactly the same path regardless of what they know, want, and are willing to invest. A distinctly Dutch ambition might look like this: a society where the average citizen has meaningful freedom to invest in their own health, without undermining the collective foundation that makes the Netherlands what it is.
That means keeping universally accessible baseline care strong, but also giving people room to take additional steps if they choose to. Not prescribing how anyone should live, but removing the barriers that currently prevent people from acting on their own health. Perhaps you choose to spend your money on travel. Perhaps on rest. Perhaps on five additional healthy years with your grandchildren. What matters is that the choice is yours to make.
What would it take?
Not necessarily more money in the system, but different choices about how the system works. More room for prevention means earlier and simpler access to screenings and diagnostics that make risks visible before symptoms appear, not after. Faster adoption of what already works means not reckless experimentation, but a willingness to act on clear evidence rather than waiting for the last percentage point of certainty. An honest distinction between baseline care and personal optimisation would mean a strong public floor for everyone, with transparent and responsible pathways for those who want to go further. And a shift in focus, from treating disease once it arrives, to helping people gain time. Years in which they can live well, stay capable, and remain present for the people around them.
None of this requires a break with Dutch values. It requires a next step within them. The foundation is already among the strongest in the world. The question is whether we'll also build the room for those who want it to do more.
.avif)
Ontvang 100 inzichten van Longevity arts Alexander Rakic voor duurzame gezondheid en prestaties



.jpeg)